Early diagnosis is critical in the appropriate management of nontuberculous mycobacterial (NTM) lung disease.1-3
The index of suspicion for NTM remains low, taking ~20 months from the first NTM-related symptom or diagnostic procedure for patients to receive an NTM lung disease diagnosis4,5
An NTM lung disease diagnosis is challenging due to its nonspecific or overlapping symptomatology in patients with underlying lung disease4,6-8
Despite increasing prevalence, the index of suspicion for NTM lung disease remains low, making early diagnosis an ongoing challenge.4,10-12
NTM lung disease can often be missed due to its nonspecific or overlapping symptomatology in patients with underlying structural lung disease, resulting in NTM being undiagnosed or misdiagnosed.1,3,6,10,11,13
If not diagnosed early enough and left unchecked, NTM lung disease can lead to a decline in lung function, worsening symptoms, and a decrease in overall quality of life for patients.3,8,9,11,14,15
In patients who meet the diagnostic criteria for NTM pulmonary disease, the latest guidelines recommend initiation of treatment rather than watchful waiting, especially in the context of positive AFB sputum smears and/or cavitary lung disease.8
A delay in diagnosis may lead to managing NTM lung disease inappropriately. For instance, many patients may have coexistent NTM and bronchiectasis, and the use of chronic macrolide monotherapy for bronchiectasis may result in macrolide-resistant NTM lung disease.1,3,8,16,17
Just hours on the timer, attention on the fire. We'll braise and flambe. It's such a glorious day. My dinner party is today.
Knives, at the ready. Pots, simmer steady. Candles on, lights put in.
All my guests will never want to leave. Just remember, this is our big shot.
My stomach is in knot.
It's so fine to wine and dine with dear old friends. They're not coming. Somehow, I cannot hide what lingers in sight. So fatigued, but I really, really tried. How like a fool I feel, thinking a single meal wouldn't become a sad ordeal. All our grand plans have trulycome undone, and my lovely dinner party is now a table for one.
People thought my cough meant I was contagious. It made me feel sad and self-conscious.
Debbie’s undiagnosed NTM symptoms made her feel isolated and alone, driving away her friends and family. Watch “Isolation,” an animation inspired by Debbie’s story.
2020 NTM TREATMENT Guidelines diagnostic criteria
The 2020 NTM Treatment Guidelines require the diagnostic criteria established in the 2007 ATS/IDSA Statement.8
Pulmonary or systemic symptoms
Exclusion of other diagnoses
Nodular or cavitary opacities on chest radiograph, or bronchiectasis with multiple small nodules on chest HRCT scan
Positive culture results from at least 2 separate expectorated sputum samples over an interval of at least a week with the same species, or
Positive culture result from at least 1 bronchial wash or lavage, or
Transbronchial or other lung biopsy with mycobacterial histologic features and positive culture for NTM or biopsy showing mycobacterial histologic features and 1 or more sputum or bronchial washings that are culture positive for NTM
NTM lung disease should be considered in the differential diagnosis of patients presenting with7,8:
Chronic pulmonary and constitutional symptoms (including chronic cough, sputum production, fatigue, and weight loss)
Nodular bronchiectatic and/or fibrocavitary features
Patients who are suspected of having NTM lung disease, but do not meet the diagnostic criteria, should be observed until the diagnosis is firmly established or excluded.8
The 2020 NTM Treatment Guidelines recommend specific management depending on radiographic presentation8
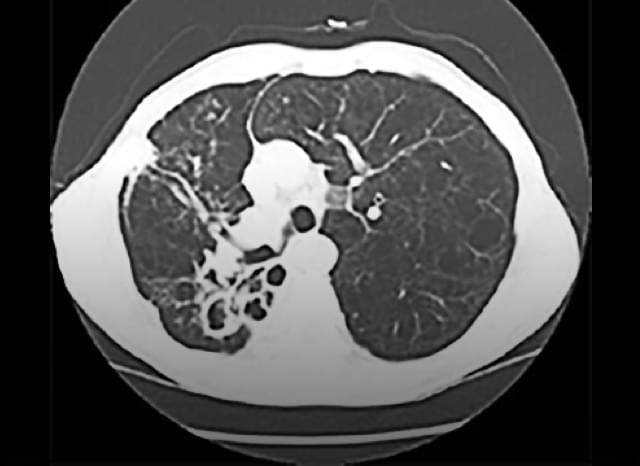
Slowly progressing form of NTM lung disease7
Presents with bilateral multilobar bronchiectasis, especially in the middle and lower lung fields4
The 2020 NTM Treatment Guidelines recommend a multidrug regimen administered 3 times per week8
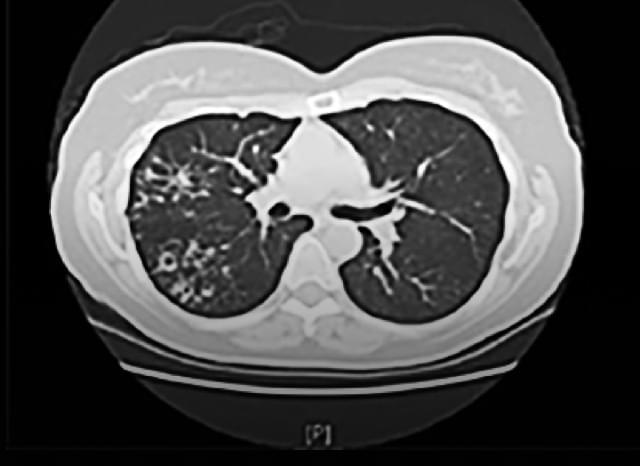
Rapidly progressing form of NTM lung disease7,8
May lead to extensive cavitary lung damage—typically in the upper lobe—as well as respiratory failure within a few years4,6,7
The 2020 NTM Treatment Guidelines recommend a multidrug regimen administered daily. Intravenous antibiotics may also be necessary8
Three years of productive cough, with yellow, brown, and occasionally blood-tinged sputum and chest pain; patient mentioned she was previously diagnosed with bronchiectasis. PCP ordered an AFB smear, which showed a positive result. As symptoms progressed, NTM lung disease was suspected and patient was referred to a pulmonologist.
Physical examination: tall, slender with scoliosis, pectus excavatum; auscultation revealed mitral valve prolapse, wheezing, and crackles
X-Ray/CT scan: showed nodular opacities with local bronchiectasis and local cystic bronchiectasis
AFB smear: positive, but negative PCR assay for Mycobacterium tuberculosis
Culture:Mycobacterium avium isolated from 3 sputum samples
Susceptibility testing: susceptible to clarithromycin
Treatment & follow-up: NTM lung disease was treated with a multidrug regimen TIW according to the 2020 NTM Treatment Guidelines
Monthly patient visits and sputum cultures
Improved clinical symptoms; sputum production became minimal
Patient was treated for 6 months and sputum AFB culture was negative previous month
Therapy should continue until patient remains culture negative for 12 months.8
One year of progressive cough with greenish sputum; treated for pneumonia with multiple antibiotics without symptomatic improvement. Patient is currently a smoker and has severe COPD. Positive sputum culture showed AFB and confirmed infection with Mycobacterium intracellulare. Patient was referred to an ID specialist with experience treating NTM.
Physical examination: overweight with wheezing and crackling on auscultation
X-Ray/CT scan:
Chest CT scan showed thin-walled cavity in right upper lobe
Severe emphysematous changes
Stable calcified nodule in right upper lobe and mediastinal lymphadenopathy
X-ray and CT scan showed cavitary lesions
AFB smear: positive
Culture: 3 positive samples identified M intracellulare
Susceptibility testing: susceptible to clarithromycin
Treatment & follow-up: NTM lung disease was treated with a multidrug regimen daily according to the 2020 NTM Treatment Guidelines
Monthly patient visits and sputum cultures
Symptoms improved; sputum production was reduced
Sputum continued to be positive for 6 months and adjustments were made to the therapeutic regimen. Four months later, his sputum was still AFB-positive but showed reduced mycobacterial burden
This treatment recommendation is consistent with the 2020 Guidelines
Therapy should continue under close monitoring with a goal to achieve sputum conversion to negative.
Dry cough for the past 4 years; diagnosed with anemia, asthma, and hyperlipidemia, with family history of TB. Previously treated for pneumonia and TB. Patient was referred to pulmonologist and was diagnosed with NTM lung disease. After treatment initiation, ocular toxicity was detected and treatment was stopped.
Physical examination: overweight with wheezing and crackling on auscultation
X-Ray/CT scan: nodular opacity and bronchiectasis
AFB smear: reported positive in 2 sputum samples
Culture:M avium isolated from 3 sputum samples
Treatment & follow-up: treatment was stopped due to potential side effects. Patient is currently stable with symptoms closely monitored
Patient visits every 3 to 6 months
Patient did not achieve culture conversion
Patient should be monitored closely for worsening symptoms.
Collecting sputum samples is a key component of the diagnosis and management of NTM lung disease. According to the 2020 NTM Treatment Guidelines, establishing an active monitoring plan that includes regular sputum cultures is recommended whether antibiotic treatment is initiated or delayed (if watchful waiting is the course of action).7,8
While the collection methods can be either invasive or noninvasive, it’s important to tailor the approach depending on the patients and if they are able to readily produce a sample.8
Noninvasive techniques
Huff cough
The huff cough requires mild to moderate forced exhalation (huff) with open glottis to help expectorate sputum18,19
Oscillation
PEP devices use collateral ventilation with oscillations to loosen mucus, which can lead to increased sputum clearance18,20
Induction
Inhalation of isotonic or hypertonic solutions administered by nebulization has been demonstrated to induce a small amount of airway secretion that can be expectorated and analyzed21
Pretreatment with a short-acting β2-agonist (dilation aid) is recommended in order to prevent excessive bronchoconstriction
The concentration of saline used for sputum induction varies by patient, ranging from 0.9% to 7.0%
Cumulative duration of nebulization should be 15 to 20 minutes using an ultrasonic nebulizer for best results
The 2020 NTM Treatment Guidelines recommend collecting ≥3 respiratory samples over at least a week to distinguish NTM lung disease from the occasional presence of NTM in the respiratory tract.8
Invasive technique
Bronchoscopy
If sputum cannot be obtained through noninvasive methods, a bronchoscopy with or without a lung biopsy may be necessary7,8
Precautions to consider before collecting a sputum sample:
Contamination can occur due to environmental exposure.8
Specimens should be submitted without fixatives.22
Collect samples in sterile, leak-proof, disposable, non-wax containers to avoid contamination, which may produce false positive smear results.22,23
Consider consulting with a respiratory therapist, as needed, for patients who are struggling to produce a viable sputum sample.24
Working with the microbiology lab
Evidence based solely on clinical and radiographic observations is not enough to establish an NTM diagnosis. According to the 2020 NTM Treatment Guidelines, correct identification of NTM is an essential component of the diagnostic process.8
Sputum sample testing procedures for NTM
Test type
Description
Culture
The 2020 NTM Treatment Guidelines recommend that all cultures for NTM include both solid and broth (liquid) media, the latter allowing higher yield and faster results. Solid media allow observation of colony morphology, growth rates, recognition of >1 mycobacterial species, and quantitation of the infecting organism.7,8,23
Most cultures should be incubated for 2 to 3 weeks, although some may need at least 8 to 12 weeks to determine the type of species and subspecies; however, rapidly growing mycobacteria usually grow within 7 days of subculture.7
AFB smear
The AFB smear test is used in conjunction with the AFB culture test. An AFB smear is a microscopic examination of a specimen that has been stained to detect acid-fast bacteria, such as NTM organisms. This test can provide probable (presumptive) results within 1-2 days.8,25
Sputum cultures should be obtained every 1 to 2 months during the treatment of MAC lung disease to assess response.8
Polymerase chain reaction (PCR)
PCR testing allows rapid detection of drug resistance through the identification of genes associated with resistance and provides preliminary guidance on effective therapy.26,27
This method is used to duplicate copies of a specific DNA sample, allowing scientists to take a very small sample of DNA, which they can then amplify and study in detail.26
REFLEX TESTING MAY BE AVAILABLE
Reflex testing refers to additional tests that are automatically performed by a laboratory when initial test results are positive or outside of normal parameters28
For example, if an AFB smear and culture are positive, the reflex testing will allow the laboratory to automatically identify the mycobacterial species without having to order species identification separately
The laboratory may include all related reflex testing under a single ordering code28
Local and regional laboratories may have their own naming conventions and codes. Contact them to understand how to order these tests.
Requesting speciation and susceptibility panels is important for NTM management decisions
The 2020 NTM Treatment Guidelines recommend identifying NTM isolates down to the species and subspecies level, and not just the group level (eg, Mycobacterium chelonae and M abscessus groups). Correct species- and subspecies-level identification is necessary to accurately assess the clinical significance and severity of isolates. Susceptibility to all relevant drugs should be established for all clinically significant isolates before treatment initiation.8,29
For example, MAC can be classified into distinct species—including M avium and M intracellulare.29-31
The species M abscessus can be further divided into 3 subspecies: M abscessus, M massiliense, and M bolletii, which are increasingly important to identify as each may impact treatment decisions.8
Proper testing procedures continue to evolve to meet the need for more rapid species identification and differentiation. Molecular methods, such as line probe hybridization, polymerase chain reaction-restriction fragment length, polymorphism analysis, and DNA sequencing, have become more popular than traditional biochemical tests or high-performance liquid chromatography.4,8,32
Rapid species and subspecies identification is paramount in order to implement the right treatment regimen.4,8,32
The correlation between in vitro susceptibility testing for MAC and clinical response has only been established for a limited number of antibiotics.8
Collect sputum: Consider the patient’s comfort level and obtain sputum through noninvasive techniques, using invasive only if necessary.8
Work with the microbiology laboratory: Send cultures and request speciation/subspeciation and susceptibility panels at the same time.8
Obtain results from the laboratory: If results cannot be obtained through a commercial laboratory, determine if the collection of additional sputum should be sent to a reference laboratory.7
Reference laboratories with additional technology that aid in NTM specimen analysis may be helpful in certain cases.7
I think one of the most important things a provider can do, whether they're an ID specialist or pulmonologist, is contact their local microbiology lab and ensure that they understand what type of testing is being performed. I think it's very important that labs are performing speciation. But additionally, it's important that they have susceptibility testing, because that helps dictate often times drug dosing as well as selection of drug type.
[MUSIC PLAYING]
Quality sample criteria
Every laboratory should have specific criteria for accepting and rejecting samples in order to ensure that optimal methods are being followed. It is incumbent on the laboratory to appropriately communicate sample requirements to the physician to ensure the best quality outcome.23
General best practices when submitting to the laboratory:
Ensure an adequate amount of specimen is collected by obtaining as much material as possible. An adequate sample of sputum should be thick unlike watery saliva with a volume of 3 mL to 5 mL per sample23
A sputum volume of <3 mL or a sample that consists mostly of watery saliva may be rejected
Taking a multidisciplinary approach
NTM lung disease treatment decisions are often difficult, and may require experience managing the disease according to the 2020 NTM Treatment Guidelines. This may mean that a peer consultation or referral to a pulmonologist or ID specialist experienced in the management of NTM lung disease is necessary.4,8,13
To find a specialist with experience managing NTM lung disease, consider the following search tools:
Kwon YS, Koh WJ. Diagnosis of pulmonary tuberculosis and nontuberculous mycobacterial lung disease in Korea. Tuberc Respir Dis (Seoul). 2014:77(1);1-5.
Maiga M, Siddiqui S, Diallo S, et al. Failure to recognize nontuberculous mycobacteria leads to misdiagnosis of chronic pulmonary tuberculosis. PLoS One. 2012;7(5):e36902.
Riello FN, Brígido RTS, Araújo S, Moreira TA, Goulart LR, Goulart IMB. Diagnosis of mycobacterial infections based on acid-fast bacilli test and bacterial growth time and implications on treatment and disease outcome. BMC Infect Dis. 2016:16:142.
Data on file. Insmed Incorporated. Bridgewater, NJ.
Young JD, Balagopal A, Reddy NS, Schlesinger LS. Differentiating colonization from infection can be difficult. Nontuberculous mycobacterial infections: diagnosis and treatment. J Respir Dis. 2007;28(1):7-18.
Griffith DE, Aksamit T, Brown-Elliott BA, et al; ATS Mycobacterial Diseases Subcommittee. An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med. 2007;175(4):367-416.
Daley CL, Iaccarino JM Jr, Lange C, et al. Treatment of nontuberculous mycobacterial pulmonary disease: an official ATS/ERS/ESCMID/IDSA clinical practice guideline: executive summary. Clin Infect Dis. 2020. doi:10.1093/cid/ciaa241.
Olivier KN, Griffith DE, Eagle G, et al. Randomized trial of liposomal amikacin for inhalation in nontuberculous mycobacterial lung disease. Am J Respir Crit Care Med. 2017;195(6):814-823.
Kotilainen H, Valtonen V, Tukiainen P, Poussa T, Eskola J, Järvinen A. Clinical findings in relation to mortality in non-tuberculous mycobacterial infections: patients with Mycobacterium avium complex have better survival than patients with other mycobacteria. Eur J Clin Microbiol Infect Dis. 2015;34(9):1909-1918.
Adjemian J, Olivier KN, Seitz AE, Holland SM, Prevots DR. Prevalence of nontuberculous mycobacterial lung disease in U.S. Medicare beneficiaries. Am J Respir Crit Care Med. 2012;185(8):881-886.
Khan Z, Miller A, Bachan M, Donath J. Mycobacterium avium complex (MAC) lung disease in two inner city community hospitals: recognition, prevalence, co-infection with Mycobacterium tuberculosis (MTB) and pulmonary function (PF) improvements after treatment. Open Respir Med J. 2010:4;76-81.
Park HY, Jeong BH, Chon HR, Jeon K, Daley CL, Koh WJ. Lung function decline according to clinical course in nontuberculous mycobacterial lung disease. Chest. 2016;150(6):1222-1232.
Mehta M, Marras TK. Impaired health-related quality of life in pulmonary nontuberculous mycobacterial disease. Respir Med. 2011;105(11):1718-1725.
Griffith DE, Brown-Elliott BA, Langsjoen B, et al. Clinical and molecular analysis of macrolide resistance in Mycobacterium avium complex lung disease. Am J Respir Crit Care Med. 2006;174(8):928-934.
Chalmers JD, Aliberti S, Blasi F. Management of bronchiectasis in adults. Eur Respir J. 2015;45(5):1446-1462.
McShane PJ, Tino G. Bronchiectasis. Chest. 2019;155(4):825-833.
McIlwaine M, Bradley J, Elborn JS, Moran F. Personalising airway clearance in chronic lung disease. Eur Respir Rev. 2017;26(143). doi:10.1183/16000617.0086-2016.
Main E, Grillo L, Rand S. Airway clearance strategies in cystic fibrosis and non-cystic fibrosis bronchiectasis. Semin Respir Crit Care Med. 2015;36(2):251-266.
Paggiaro PL, Chanez P, Holz O, et al. Sputum induction. Eur Respir J. 2002;20(Suppl37);3s-8s.
Griffith DE, Eagle G, Thomson R, et al. Amikacin liposome inhalation suspension for treatment-refractory lung disease caused by Mycobacterium avium complex. Online data supplement. Am J Respir Crit Care Med. 2018;198(12)(suppl):E1-E28. Accessed May 28, 2020. https://www.atsjournals.org/doi/suppl/10.1164/rccm.201807-1318OC/suppl_file/griffith_data_supplement.pdf.
Forbes BA, Hall GS, Miller MB, et al. Practice guidelines for clinical microbiology laboratories: mycobacteria. Clin Microbiol Rev. 2018;31(2):e00038-17.
Polverino E, Goeminne PC, McDonnell MJ, et al. European Respiratory Society guidelines for the management of adult bronchiectasis. Eur Respir J. 2017;50(3). doi:10.1183/13993003.00629-2017.
Lab Tests Online. American Association for Clinical Chemistry. Acid-fast bacillus (AFB) testing. Modified July 22, 2020. Accessed August 10, 2020. https://labtestsonline.org/tests/acid-fast-bacillus-afb-testing.
Wages JM Jr. Polymerase chain reaction. Encyclopedia of Analytical Science. 2005:243-250. doi:10.1016/B0-12-369397-7/00475-1.
Frickmann H, Masanta WO, Zautner AE. Emerging rapid resistance testing methods for clinical microbiology laboratories and their potential impact on patient management. Biomed Res Int. 2014:375681. doi:10.1155/2014/37561.
Office of the Federal Register. Laboratory requirements. In: Electronic Code of Federal Regulations. Title 42; IV; 493. Updated July 1, 2020. Accessed July 6, 2020. www.ecfr.gov.
Boyle DP, Zembower TR, Reddy S, Qi C. Comparison of clinical features, virulence, and relapse among Mycobacterium avium complex species. Am J Resp Crit Care Med. 2015;191(11):1310-1317.
Johnson MM, Odell JA. Nontuberculous mycobacterial pulmonary infections. J Thorac Dis. 2014;6(3):210-220.
Shin SJ, Lee BS, Koh WJ, et al. Efficient differentiation of Mycobacterium avium complex species and subspecies by use of five-target multiplex PCR. J Clin Microbiol. 2010;48(11):4057-4062.
El-Zeenni N, Chanoine S, Recule C, Stahl JP, Maurin M, Camara B. Are guidelines on the management of non-tuberculous mycobacteria lung infections respected and what are the consequences for patients? a French retrospective study from 2007 to 2014. Eur J Clin Microbiol Infect Dis. 2018;37(2):233-240.